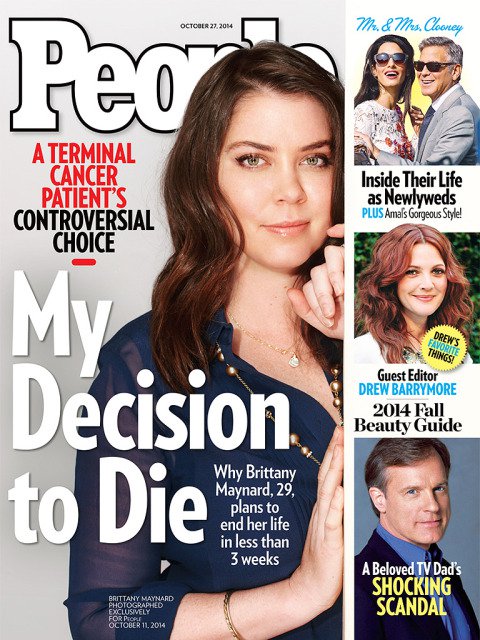
Brittany Maynard, a 29-year-old with terminal brain cancer learned that her tumor had returned once again, but in a more aggressive state. Her doctor had informed her that since her tumor was so large, she would have to proceed with the treatment of full brain radiation. The impacts of this prescribed treatment were not something she wished to endure as the side effects were extremely harsh. It would cause her to lose all her hair, leave first-degree burns on her scalp, and her quality of life would diminish – all just to give her an approximate extension of six months of life. Brittany stated that “after months of research, my family and I had reached a heartbreaking conclusion: There is no treatment that would save my life, and the recommended treatments would have destroyed the time I have left” (Maynard, 2014). Once she came to these terms, she chose to end her life with death with dignity, in particular, physician-assisted suicide. Before she actually ingested the medicine that killed her, she wrote: “If you find yourself walking a mile in my shoes, I hope that you would at least be given the same choice and that no one tries to take it from you” (Maynard, 2014).
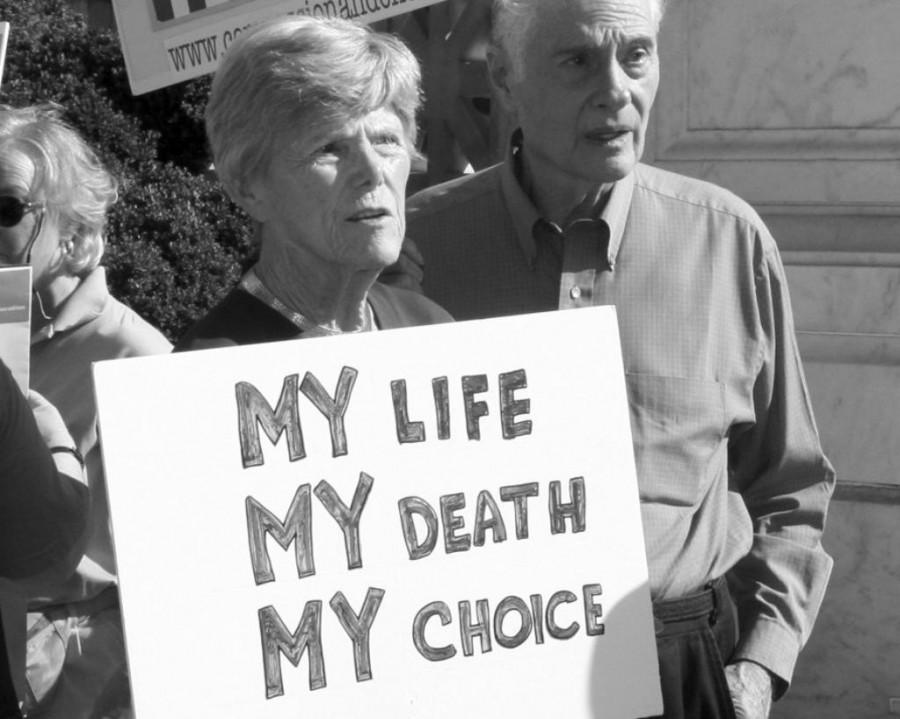
I want dignity. You want dignity. Most of all, people who are terminally ill would like dignity while they die. In the past few decades, the question over whether or not physicians should be allowed to participate in the practice of euthanasia or physician-assisted suicide to speed up the death of incurable patients has been debated. “Death with dignity laws, also known as physician-assisted dying or aid-in-dying laws, stem from the basic idea that it is terminally ill people, not the government and its interference, politicians and their ideology, or religious leaders and their dogma, who should make their end-of-life decisions and determine how much pain and suffering they should endure” (Death with Dignity Acts, 2019). Throughout this research report, I will be examining the implementation of the practice of euthanasia and physician-assisted suicide between the two countries of the United States and the Netherlands. I will be arguing that an individual’s decision on their right to choose to end their life will not only stem from their individual choice, but also their family’s perspective, their religious and physicians views, and whether or not their government has laws on this making this intervention legal to do so or not.

To be clear, physician-assisted suicide and euthanasia are related in the means that they both end in death for the terminally ill patient. For this reason, it is common for people in the United States to merge these two definitions together. However, there are clear distinctions between these two practices that should be noted. By definition, physician-assisted suicide is when “the medical provider supplies – but does not administer – life-ending narcotics to a suicidal patient” (Serlin, Reiss & Adams, 2015). Regarding euthanasia, there are two methods of intervention: active and passive. In active euthanasia, “the medical provider prescribes and then directly administers a life-ending substance” (Serlin, Reiss & Adams, 2015). Whereas involuntary passive euthanasia “entails removing medical technology that had been keeping the patient alive”, which is commonly known as “pulling the plug” (Serlin, Reiss & Adams, 2015).

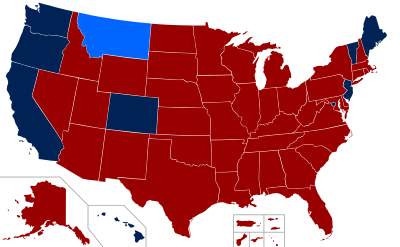
In the United States, the Supreme Court ruled that euthanasia or physician-assisted suicide is not a constitutional right or constitutionally prohibited, which allowed each state to deem whether it was legal or not in 1997 (Emanuel, 2002). In other words, this allows individual states in the US to decide what they wanted to be done with this act and not the government as one making this choice. With the Death and Dignity Act, Oregon proceeded with this choice and became the first state to legalize euthanasia and physician-assisted suicide in that same year of 1997. Typically, anywhere from 34% to 65% of the American public agree with legalizing these practices involved with the Death and Dignity Act, so it is not surprising that Oregon passed it right away (Emanuel, 2002). These percentages have remained the same, but it usually ranges above fifty percent. Now to presently in 2019, seven more states have followed the path Oregon started by legalizing their own versions of the law. In fact, just on June 12th of 2019, Maine became the eighth state to legalize physician-assisted suicide. An increasing amount of states each year are looking more in-depth into making this law legal, New York is one of them.
After states decide to legalize the practice(s), they then hold the obligation to make, regulate and oversee the rules regarding the procedure. They vary between each state, but the regulations must be strictly adhered to. For example, the eligibility, evaluation, residency, request, waiting period, and ingestion of medicine all differ from state to state. With the strict residency laws that are enforced, some people in the United States will even make the decision to move, so they then reside in a different state that would allow obtaining the medical care they prefer. This requirement can add to the stress of the family going through a difficult time.
The standards are very strict in the US, but the Netherlands is even more stern. Instead of having the Death with Dignity Acts, they have the Dutch Termination of Life on Request and Assisted Suicide Act (De Jong & van Dijk, 2017). In 2002, the Dutch Parliament gave legislative ratification to these practices with this Act. However, the killing is still illegal and punishable if committed by a doctor who has not complied with two stated conditions. The first is that “the doctor must act in accordance with the ‘requirements of careful practice’. The requirements state: 1) the doctor must be convinced that the patient had made a voluntary and well-considered request; 2) the doctor must be convinced that the patient’s suffering is hopeless and unbearable; 3) the doctor must have informed the patient about the situation; 4) both doctor and patient must be convinced there is no reasonable alternative solution to the situation; 5) the doctor must have consulted at least one other independent doctor and 6) the ending of life must be carried out with due to medical care” (Weyers, 2006). The second condition is that “the doctor must report the behavior to the coroner in accordance with a form that is specified. The report is then sent to an ‘assessment committee’, which judges whether that doctor has fulfilled the requirements of careful practice” (Weyers, 2006). These requirements obtain to everyone in the Netherlands and it is clear to see how it must be handled with extreme due process in care.
In both countries though, there have been organizations that have been formed to try and advocate for the right one should have on these practices. In the Netherlands, a group was formed called the Dutch Right to Die Society. The Society’s key objective is to “enhance freedom of choice at the end of life” (Pauline, 2019). In 2012, it successfully formed and founded the ‘End-of-Life Clinic’ where patients can go to utilize euthanasia within the limits of the law if their physician rejected their request (Willems, 2000). In the United States, the largest known organization is the Death with Dignity National Center and Death with Dignity Political Foundation. Their missions are to promote death with dignity laws based on the model legislation to provide an option for dying individuals and to stimulate nationwide improvements in end-of-life care.
Even with these Acts in place in both countries, physicians views can have a great impact on the practices. A physician’s viewpoint on these two practices can make or break a patients choice. An important difference that emerges from studies is that “American physicians seem to be much less supportive of euthanasia than their Dutch colleagues, but the support for physician-assisted suicide is very similar” (Willems, 2000). Those results may show why euthanasia has a higher percentage (4.5%) of deaths in the Netherlands compared to the United States (Pauline, 2019). Another big difference is the percentage of physicians that accept the patient’s unwillingness to be a burden to their family as an acceptable reason to end their life. Regarding physician-assisted suicide, the percentages of physicians to accept the feeling of being a burden is compared to 24% US physicians and 9% of Netherland physicians (Willems, 2000).
The feeling of being a burden is usually regarded towards the terminally ill patient’s caregivers, which are most likely members of their family. When you are terminally ill and declining rapidly, the patient usually loses their independence as they start having to depend on others for tasks. In order to care for the terminally ill, the cost of healthcare and the loss of income can become a burden impacting their choice of wanting to end their life. It should be noted that in the “in the American health care financing system, long-term palliative care may rapidly become a heavy financial burden to families of patients” (Willems, 2000). Whereas in the Netherlands, their healthcare system has shown to financially assist more even in these practices, if that’s the patients wish. It also has been studied that caregivers overall are more likely to support euthanasia or physician-assisted suicide for their loved ones. This is because the caregiver understood that there was no cure for the patient and also no quality of life filled with pain as opposed to if they opted for a natural death (Emanuel & Fairclough, 2000). Caregivers whose lives were significantly altered caring for the patient would also be even more likely to support death with dignity (Emanuel & Fairclough, 2000). Although, in some cases, some family members are against the patients choice for many reasons. This may be due to associations with Right-to-life groups, those who represent the disabled or a big reason being religious affiliations that disapprove of dying in this manner.

Religious individuals are more likely to oppose euthanasia or physician-assisted suicide (Emanuel & Fairclough, 2000). With that being said and noted that America is one of the most religious countries, being they tend to have more opposition to these practices when one is Christian. A study showed that the percentage of physicians differed between the two countries. Americans that were religious was 53% compared to 29% of the Netherland population (Willems, 2000). If the physician’s religious views impact their practice, they would be less likely to comply with the patient’s request. This could be because one of the ten commandments in the Bible it is stated that thou shall not kill.
Such as religion, certain demographics variables consistently predict support or opposition for euthanasia and physician-assisted suicide. Another factor shown to oppose one’s choice is the race of a person. The reason is unknown, but African Americans have strong resentments towards these practices. It has been shown that a high percentage in a study concluded that 88% of African American caregivers opposed their patient dying in these manners (Emanuel & Fairclough, 2000).
People who chose to end their life through the means of euthanasia or physician-assisted suicide have societal effects on themselves, their caregivers, physicians, government and health care systems. There have been many studies on these various institutions which favor and oppose dying with dignity. One of the largest oppositions is the so-called “slippery slope argument: if euthanasia were legalized it cannot be efficiently monitored and controlled and will lead to error, abuse, and the violation of the rights of vulnerable patients (Smets, 2009). The Netherlands have regulated their approved Act so that this will not happen. However, in the United States, it is up to the state to enforce how sternly they regulate the systems. Legalized or not, it is destined that these practices will become an increasingly talked about the debate as medical advances continue, people’s lives are extended, healthcare is increased in cost, and more and more people are wishing to die at home rather than institutions such as in a hospital or nursing home.
What are your views on legalizing PAS?
If one of your family members was terminally ill and wanted to die via death with dignity (PAS or euthanasia)…would you oppose their request?
Works Cited
Bristo, M., & Burgdorf Jr., R. L. (1998). Assisted suicide: A disability perspective. Issues in Law & Medicine, 14(3), 273. Retrieved from http://search.ebscohost.com.ezproxy.siena.edu:2048/login.aspx?direct=true&db=buh&AN=1515860&site=eds-live
De Jong, A., & Van Dijk, G. (2017). Euthanasia in the Netherlands: Balancing autonomy and compassion. doi:10.3897/bdj.4.e7720.figure2f
Emanuel, E. J. (2002). Euthanasia and physician-assisted suicide: a review of the empirical data from the United States. Archives Of Internal Medicine, 162(2), 142–152. Retrieved from http://search.ebscohost.com.ezproxy.siena.edu:2048/login.aspx?direct=true&db=cmedm&AN=11802747&site=eds-live
Emanuel, E. J., Fairclough, D. L., & Emanuel, L. L. (2000). Attitudes and Desires Related to Euthanasia and Physician-Assisted Suicide Among Terminally Ill Patients and Their Caregivers. JAMA, The Journal of the American Medical Association, (19). Retrieved from http://search.ebscohost.com.ezproxy.siena.edu:2048/login.aspx?direct=true&db=edsgao&AN=edsgcl.67320079&site=eds-live
King, D. A., Kim, S. Y. H., & Conwell, Y. (2000). Family matters: A social systems perspective on physician-assisted suicide and the older adult. Psychology, Public Policy, and Law, 6(2), 434–451. https://doi-org.ezproxy.siena.edu/10.1037/1076-8971.6.2.434
Maynard, B. (2014, November 03). My right to death with dignity at 29. Retrieved from http://www.cnn.com/2014/10/07/opinion/maynard-assisted-suicide-cancer-dignity/index.html
Pauline S. C. Kouwenhoven, Ghislaine J. M. W. van Thiel, Agnes van der Heide, Judith A. C. Rietjens, & Johannes J. M. van Delden. (2019). Developments in euthanasia practice in the Netherlands: Balancing professional responsibility and the patient’s autonomy. European Journal of General Practice, (1), 44. https://doi-org.ezproxy.siena.edu/10.1080/13814788.2018.1517154
Physician-Assisted Suicide: A Topic of Growing Importance. (2012, July 31). Retrieved from https://www.sociologylens.net/topics/science-technology/physician-assisted-suicide-a-topic-of-growing-importance/10335
Serlin, D., Reiss, B., & Adams, R. (2015). Keywords for Disability Studies. New York: NYU Press. Retrieved from http://search.ebscohost.com.ezproxy.siena.edu:2048/login.aspx?direct=true&db=nlebk&AN=992496&site=ehost-live
Smets, T., Bilsen, J., Cohen, J., Rurup, M. L., De Keyser, E., & Deliens, L. (2009). The medical practice of euthanasia in Belgium and The Netherlands: legal notification, control and evaluation procedures. Health Policy (Amsterdam, Netherlands), 90(2–3), 181–187. https://doi-org.ezproxy.siena.edu/10.1016/j.healthpol.2008.10.003
Weyers, H. (2006). Explaining the emergence of euthanasia law in the Netherlands: how the sociology of law can help the sociology of bioethics. Sociology of Health & Illness, 28(6), 802–816. https://doi-org.ezproxy.siena.edu/10.1111/j.1467-9566.2006.00543.x
Willems DL, Daniels ER, van der Wal G, van der Maas PJ, Emanuel EJ. (2000) Attitudes and Practices Concerning the End of Life: A Comparison Between Physicians From the United States and From the Netherlands. Arch Intern Med. 2000;160(1):63–68. doi:10.1001/archinte.160.1.63

Hi Brittney,
Your topic was very fascinating to read about as it had been a hot topic for so many years now. I remember having debates about these practices in high school and even back then things would get heated. I was most intrigued by how you differentiated physician-assisted suicide and involuntary passive euthanasia. When I read about involuntary passive euthanasia, I essentially thought of hospice care and how basically you are weaned off life support little by little until the end. I’m unsure if these two concepts are related by any means but now I am definitely going to research it on my own! I was surprised however that euthanasia and physician-assisted suicide is not a “constitutional right.” Cohen mentioned life expectancy in Chapter 2 by writing, “today more than ¾ of Americans live to age 75. This increased longevity is the result of improvements in the standard of living, including sanitation, medical care, and nutrition” (Cohen 2015, pg. 33). However, the story you mentioned at the beginning of your post leads me to believe that even the best medical care may be detrimental to our overall well-being in all spheres (physical, emotional, mental, spiritual). I believe this is a choice that the individual should be able to make for themselves under the care of their medical team, not the government.
LikeLike
Hi Brittney,
I enjoyed reading your post I think its a topic that the United States should be discussing more frequently. I might be biased because this idea of physician assisted suicide hits closer to home for me. My mom had terminal cancer and was only given weeks to live and for most of it she was in the hospital or in hospice, which can be costly if people do not have good insurance. I like the idea of dying with dignity because I know she didn’t enjoy having to rely on her family take care of her for everything, even going to the bathroom. Its crazy to think that when people aren’t getting divorced in marriages, the other “47 percent are ending with the eventual death of one of the spouses” (369). I think having physician assisted suicide could be easier for the family as well so the grieving process can begin earlier rather than waiting for the eventual death.
LikeLike